Δευ: 18:30 – 21:30 - Τετ:18:30 – 21:30 - Παρ:18:30 – 21:30
Δερβενακίων 30 & Υγείας, Παλλήνη
The technique of autologous chondrocyte transplantation flourished in the late 90s and was developed by PETERSON in 1994.
Already in large, specialized centers abroad, such as the Royal National Orthopaedic Hospital, Stanmore, in London, this technique has been in use for over 11 years, with very good results in a large number of patients.
Indications for ACM (autologous chondrocyte transplantation):
The ACM method includes 2 stages.
 |
 |
||
|
How does the lesion appear in arthroscopy
|
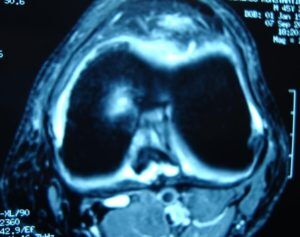
Image of the lesion in MRI
|
Contraindications for the application of the method:
From a scientific point of view, the AMX has a comparative theoretical advantage in terms of creating better hyaline articular cartilage over time.
However, it is technically demanding, requires 2 surgical sessions and its cost is still high.
A necessary prerequisite for success is of course its application by an experienced and specially trained Orthopaedic Surgeon.
It also requires a continuous and long-term physiotherapy rehabilitation program.
The overall recovery program is completed in approximately 18 months.
 copy")
